The Frontal Lobe
Thge Common Vein Copyright 2010
Definition
The frontal lobe is the foremost portion of the brain and is part of the forebrain. It is located at the front of the cerebral hemisphere and in front of the temporal and parietal lobes.
Structurally it is characterized by being the largest and most anterior part of the forebrain. The frontal lobe is all the portion of the external face of the hemisphere anterior to the central fissure. It contains three fissures (the precentral, superior and inferior frontal sulci) that separate four convolutions (superior, middle, and inferior frontal gyri as well as the precentral gyrus).
Functionally it has a major role in executive thought processes and decision-making behavior. . It includes the motor, premotor and prefrontal cortex. It is involved in setting up actions and skeletal movement as well as abstract thought. The activity in the frontal lobe increases when a difficult task needs to be done more efficiently. The front of the frontal lobe – the prefrontal cortex – is responsible for the strategy, ie, sequencing of movements and evaluation of its outcome.
The frontal lobe is vital for many motor and “higher cortical” functions and these functions are represented in various areas of the frontal cortex. Examples include the motor homunculus which is a somatotopical map of the various contralateral body parts and their respective areas of motor representation.
The frontal lobe also contains important areas for speech, particularly, in the dominant hemisphere, Broca’s area, which functions as the motor area for speech. A part of the frontal lobe is also responsible for conjugate eye movements, and is known as Brodmann’s area 8.
The prefrontal cortex is responsible for abstract and creative thinking, language, emotional responses, capacity for social connections and selective attention.
Disease and dysfunction in this area can lead to schizophrenia and severe depression as well as personality and emotional changes.
Changes in the frontal lobe can result in attention, concentration and motivation deficits; increased impulsivity and disinhibition; loss of self control, difficulties in recognizing guilt; loss of insight – symptoms positively correlated with criminal behavior – and inability to learn from experience.
Trauma to the prefrontal cortex make a person get stuck persistently to strategies that do not work, since they lose the ability to develop a correct sequence of actions. Since the frontal lobe is responsible for the motor planning, it follows that a damage to it may result in contralateral weakness, spasticity and paralysis.
Diagnosis involves completion of various general cognitive response tests as well as tests for specific cognitive deficits.
Treatment is psychiatric, medical and less commonly surgical.
The Frontal Lobe (lime green) Part of the Forebrain (Prosencephalon) Member of the Cerebrum (Telencephalon) Member of the Cereberal Hemispheres |
|
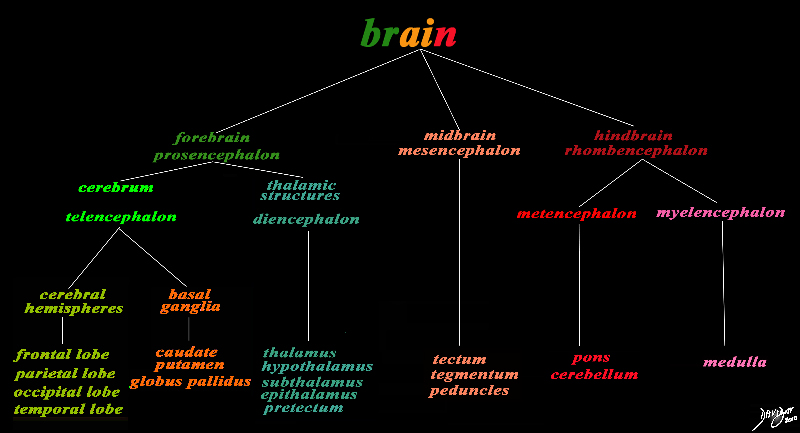
The basic and simplest classification of the brain into forebrain midbrain and hindbrain is shown in this diagram and advanced to a more complex tree using the embryological and evolutionary terminologies. The forebrain consists of the cerebrum also called the prosencephalon, which contains the more advanced form of the brain and the thalamic structures which contain more basic structures. The cerebrum (telencephalon) itself consists of two cerebral hemispheres and paired basal ganglial structures. Each cerebral hemisphere will have gray and white matter distributed in the frontal parietal temporal and occipital lobe, with the basal ganglia being part of the gray matter deep in the cerebral hemispheres. The most important thalamic structures arising from the diencephalons include the thalamus itself and the hypothalamus. The midbrain (mesencepaholon) consists of the tectum tegmentum and cerebral peduncles. The hindbrain has two major branch points based on the evolutionary development. The pons and cerebellum(part of the metencephalon) are grouped and the medulla (part of the myelencephalon is the second branch. Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 97686.8s |
|
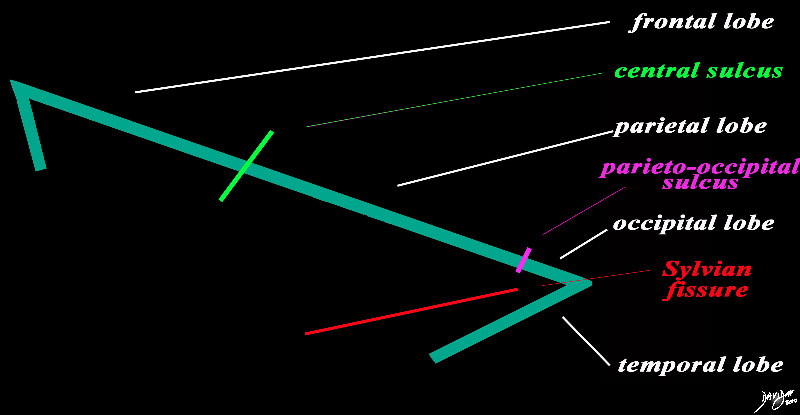
The Central Sulcus is the Border between the Frontal Lobe and the Parietal Lobe |
|
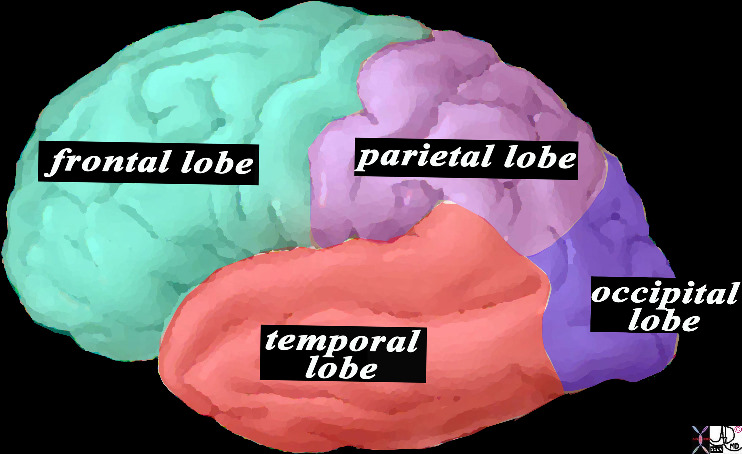
The forebrain is divided into the frontal lobe anetriorly, separated by the central sulcus (bright green), the parietal lobe separated from the occipital lobe by the parieto-occipital fissure (pink), and the temporal lobe separated from the frontal and occip[ital lobe by the Sylvian fissure (lateral sulcus) (red). The distinction between the occipital and temporal lobe is more of a functional division than a structural division Courtesy Ashley Davidoff MD copyright 2010 93887b03b05.8s |
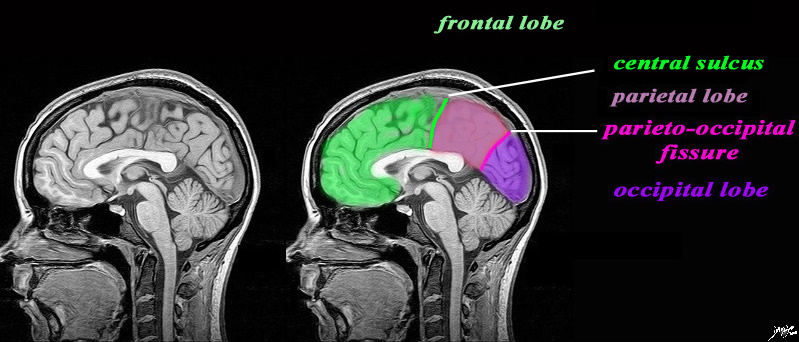
MRI Showing the Central Sulcus and the Lobes |
|
The sagittal image is deeper in the brain near the midline through the interhemispheric fissure, and is intended to demonstrate the the parieto-occipital fissure (pink) in order to define the border between the parietall and occipital lobe. The central sulcus (pink) has also been inferred in to demonstrate the border between the frontal lobe and parietal lobe. It is not usually seen in this projection. The Sylvian is also not usually seen in this projection. What we do start to appreciate are the layers of inverted c shaped structures. MRI 3D FFE Courtesy Philips Medical systems rendered by Davidoff art 92141c01label.82s |
83029d13.8s |
|
This is a diagram looking at the forebrain from the side showing the anteriorly placed frontal lobe, inferiorly placed temporal lobe posteriorly placed occipital lobe and superiorly placed occipital lobe. In this view the size of the frontal lobe dominates and in fact it is the largest portion of the forebrain. Courtesy Ashley DAvidoff MD copyright 2010 all rights reserved 83029d13.8s |
Parts of the Frontal Lobe |
| 83029b01b01b03.8s brain somatosensory cortex parietal lobe medial longitudinal fissure medially central sulcus anteriorly postcentral sulcus posteriorly lateral sulcus inferiorly location of primary somatosensory cortex main sensory receptive area touch. maps sensory space homunculus in this location pink = somatosensory cortex in post central gyrus light blue blue = primary motor cortex dark blue = premotor cortex purple fuschia = prefrontal cortex The Common vein Davidoff art copyright 2008 |
Axial Framework of the Forebrain |
|
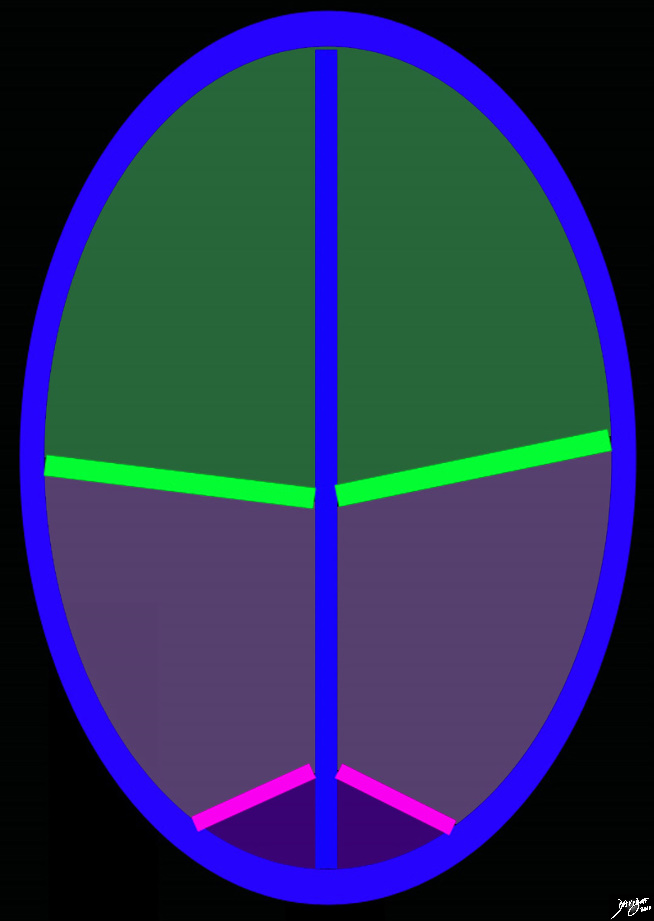
The diagram reflects the interhemispheric fissure as depicted in the axial plane dividing the brain into two halves. The bright green line represents the central sulcus which separates the the frontal lobes (green) from the parietal lobes (light purple. The parito-occipital fissure (pink) separates the parietal lobes from the occipital lobes. By convention anterior is on the top and posterior on the bottom, while the patients right is to our left and vice versa for the patients left Copyright 2010 Courtesy Ashley Davidoff MD 93914.85sb |

52981b05.8.44kb01c06.9c |
|
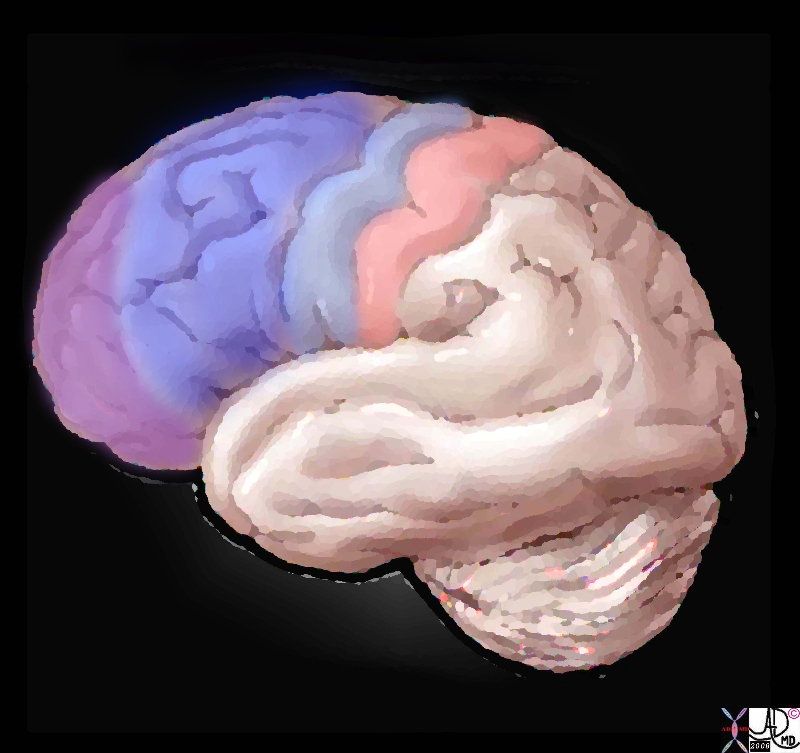
The diagram of the brain as viewed from above shows the interhemispheric fissure, and the central sulcus (lime green) which divides tyhe brain into the frontal lobe anteriorly and the parietal lobe posteriorly. The presentral gyrus, (blue) is the motor gyrus and is a landmark posterior border of the frontal lobe. The post central gyrus (pink) is the sensory gyrus and is the landmark anterior border of the parietal lobe. Copyright 2010 All rights reserved 52981b05.8.44kb01c06.9c |
|
Axial Projection MRI |
|
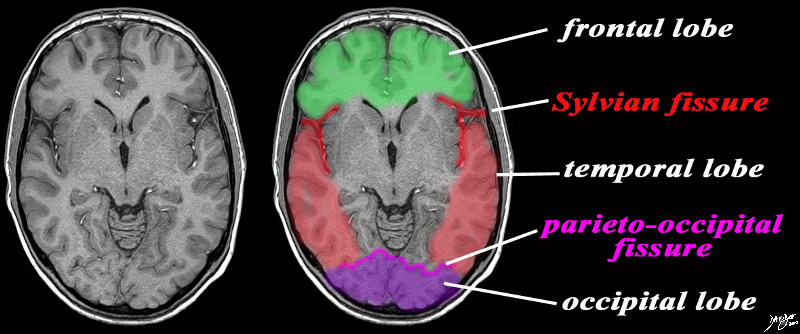
The axial image is intended to demonstrate ttwo important fissures; the Sylvian fissure (in red) the parieto-occipital fissure (pink) in order to demonstrate the border between the frontal and temporal lobe in the axial plane and the junction of the temporal and occipital lobe MRI SENSE Courtesy Philips medicaL systems rendred by Davidoff art 92142c06b01 label.8s |
The Prefrontal Cortex |
|
The prefrontal cortex of the brain is the anterior part of the frontal lobes and is positioned anterior to motor and premotor areas. It is divided into the lateral, orbitofrontal and medial prefrontal areas, Functionally it is said to have executive function in that it orchestrates thoughts and actions, discriminates between good and bad, positive and negative . It is responsible for planning, cognitive behaviors, personality expression and moderating correct social behavior. Executive Function relates to abilities to differentiate among conflicting thoughts, determine good and bad, better and best, same and different, future consequences of current activities, working toward a defined goal, prediction of outcomes, expectation based on actions, and social “control” (the ability to suppress urges that, if not suppressed, could lead to socially unacceptable outcomes). Courtesy Ashley Davidoff MD copyright 2008 38568c02.8s |
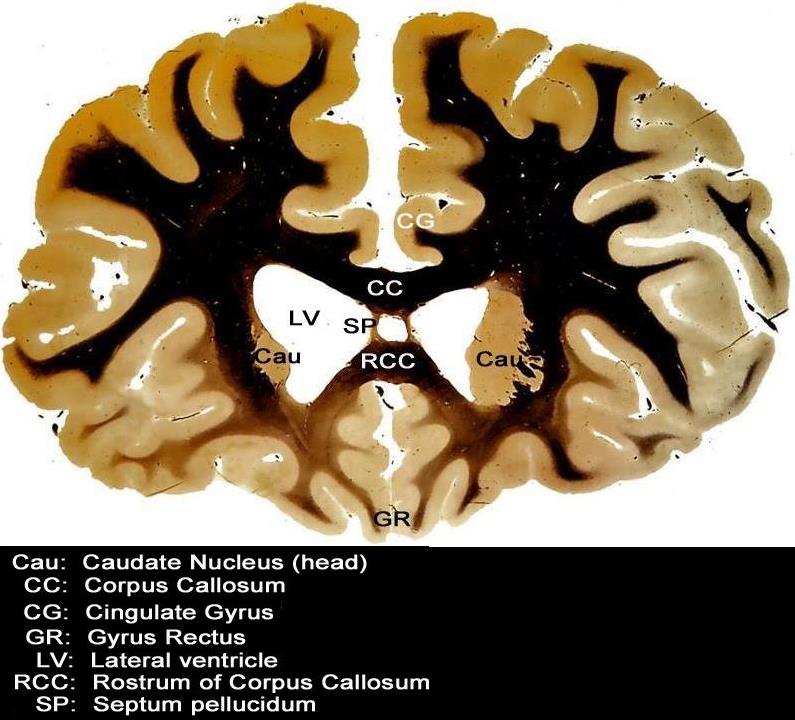
Frontal Lobe in Coronal Plane |
|
This coronal section through the forebrain is an anterior cut through the frontal lobes recognized by absence of the temporal horns, the presence of the rostrum of the corpus callosum (RCC), the cingulate gyrus (CG) superiorly and the gyrus rectus (GR) inferiorly. The visualized cortex is therefore part of the frontal lobe, and the ventricles (LV) that are visualized represent the frontal horns. The caudate nuclii (CN) are seen inferolateral to the frontal horns, and the septum pellucidum is seen medially Courtesy Department of Anatomy and Neurobiology at Boston University School of Medicine Dr. Jennifer Luebke, and Dr. Douglas Rosene 97342.C3.8L01 |
Function
The frontal lobe is vital for many motor and and “higher cortical” functions and these functions are represented in various areas of the frontal cortex. Examples include the motor homunculus which is a somatotopical map of the various contralateral body parts and their respective areas of motor representation. The frontal lobe also contains important areas for speech, particularly, in the dominant hermisphere, there is Broca’s area, which functions as the motor area for speech. A part of the frontal lobe is also responsible for conjugate eye movements, and is known as Brodmann’s area 8.
Applied Anatomy
Acute Infarction
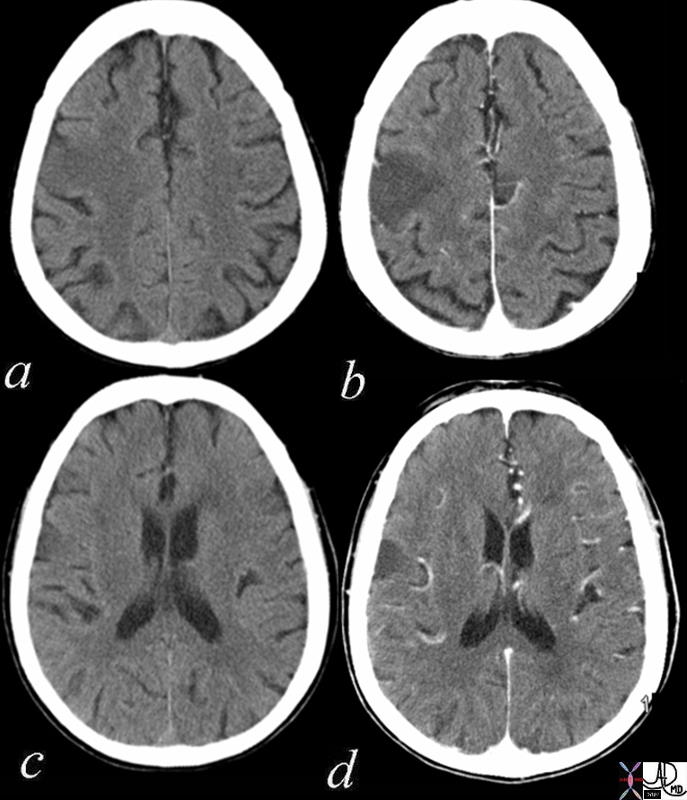
Acute Non hemorrhagic Infarction Fronto-parietal Region |
|
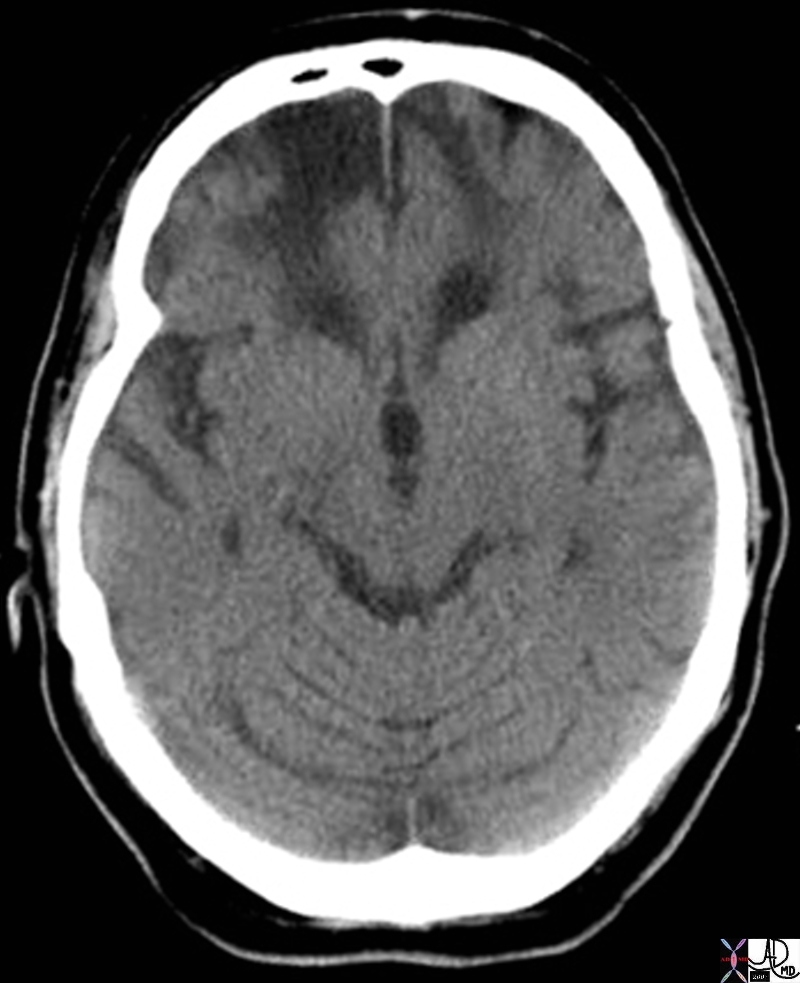
Thie axial CT scan through the ventricles is from a 73year old female with acute left sided weakness and slurred speech. Images a nd c are without contrast and images b and d are following intravenous contrast. In the right fromntoparietal region within the location of the pre and post central gyrus there is a focal hypodense region accentuated in the contrast study, with loss of the gray white differentiation, consistent with an acute infarction in the parietal lobe. Courtesy Ashley Davidoff Copyright 2010 71253c01 |
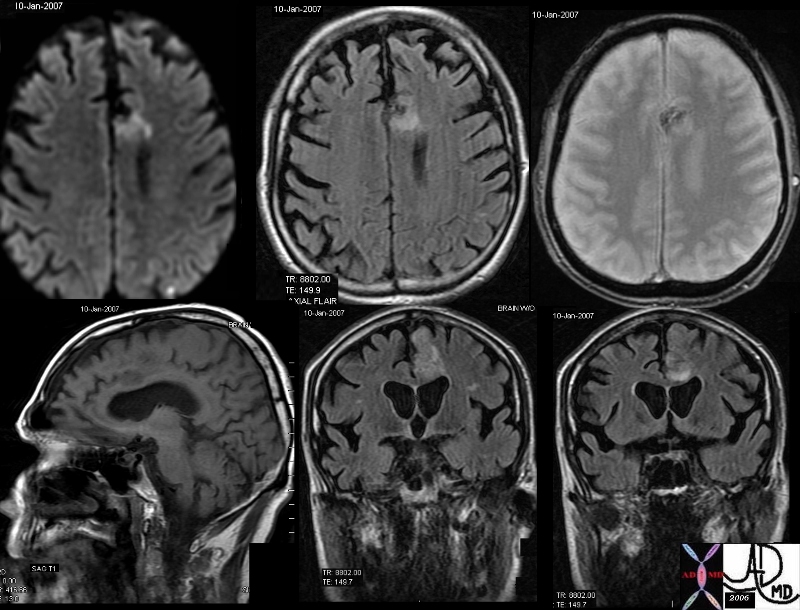
Acute Hemorrhage |
|
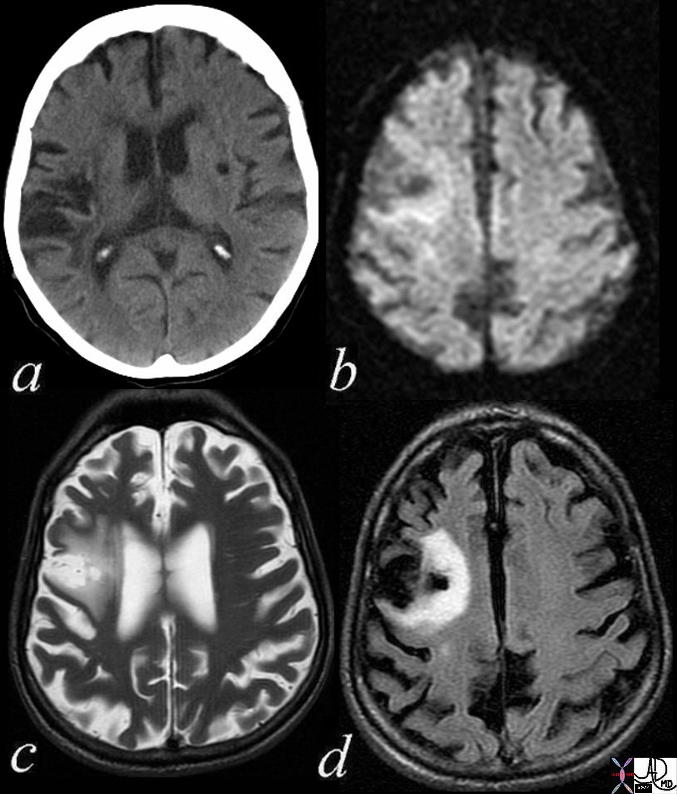
The MRI in various projections confirms the presence of an acute hemorrhagic infarct in the left paracentral frontal territory. The diffusion images (top left), show a hyperintense focus in the left frontal lobe, which is hyperintense on the axial FLAIR image (middle top), hypointense and granular on the GRE (top right), hypointense on the sagittal T1 (bottom left) and seen as hyperintense on the last two STIR coronal images. These findings are consistent with an acute hemorrhagic focus which and was thought to be embolic in origin due to other noted foci. Courtesy Ashley Davidoff MD copyright 2010 46098c01.800 |
Bilateral Chronic Frontal Infarcts |
|
The axial CT through the inferior aspect of the frontal lobes show blateral low density regions in the frontal lobes with volume loss indicative of chronic infarctsa bilaterally with encephalomalacia brain cerebral cortex cerebrum anterior and medial frontal lobe fx bilateral hypodensity bilateral chronic infarction CTscan Courtesy Ashley Davidoff MD Copyright 2010 71404 |
Chronic Infarction |
|
The MRI from a 91 year old male patient with a chronic infarction in the region of the Sylvian fissure. Image a is an axial CT scan tha shows hypodensity in the region of the Sylvian fissure with an expanded Sylvian fissure due to volume loss in the region of the insular cortex (insula) with secondary enlargement of the Sylvian fissure as a result of loss of tissue, caused by gliosis and encephalomalacia of the insular cortex Image b is a DWI image that shows T2 shine through and no acute hemorrhage. In image c is an axial T2 weighted image shows the hyperintense expanded Sylvian fissure surrounded by the less intense chronic infarct in the cerebral tissue. The border between the expanded fissure and the infarcted tissue is ill defined. Image d is an axial FLAIR image showing the process of gliosis and FLAIR intensity of chronic infarction. The distinction between the expanded Sylvian fissure and the diseased cerebral tissue is quite clear. The deformity of the lateral ventricle indicates ex vacuo change and encephalomalacia male brain cerebrum right frontal lobe extending between the Sylvian fissure and precentral gyrus white matter and medially to the surface of the lateral ventricle shape deformity of the lateral ventricle indicating ex vacuo change and encephalomalacia no abnormal enhancement Courtesy Ashley Davidoff MD Copyright 2010 All rights reserved 71559c02 |
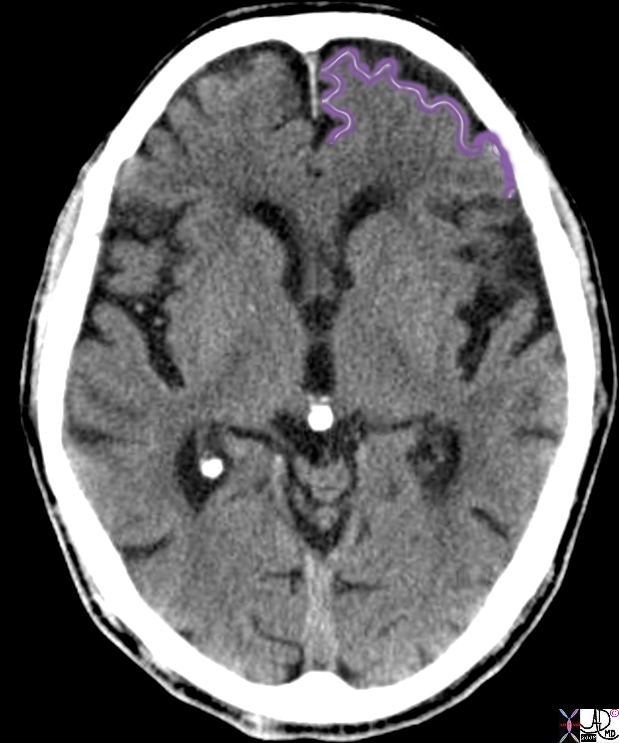
Atrophy Ex Vacuo Change and Encephalomalacia |
|
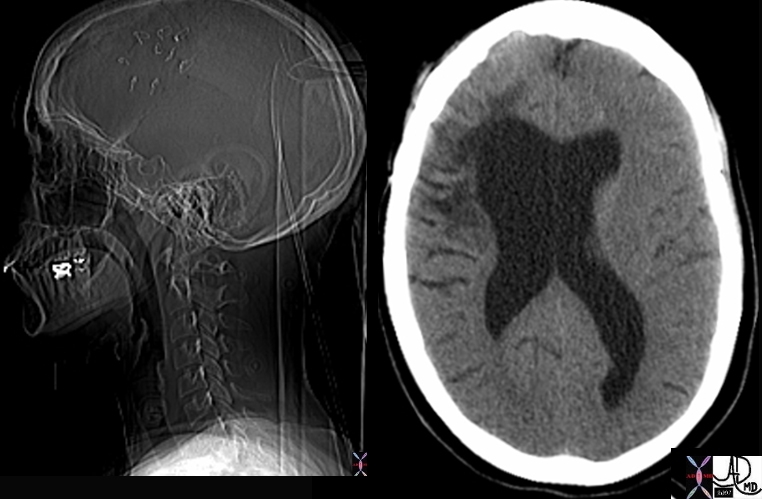
The scout film prior to a CT and the axial CT is from a young woman who sustained brain trauma following a motor vehicle accident requiring a craniotomy (surgical staples in frontoparietal bone – left image). The axial image shows loss of frontal lobe tissue and secondary changes in the right frontal horn asa result of the tissue loss with expansion of the ventricle, ex vacuo changes due to the encephalomalacia. Hypodense changes reflect the tissue damage. Courtesy Ashley Davidoff MD copyright 2010 49675c01 |
Infection
|
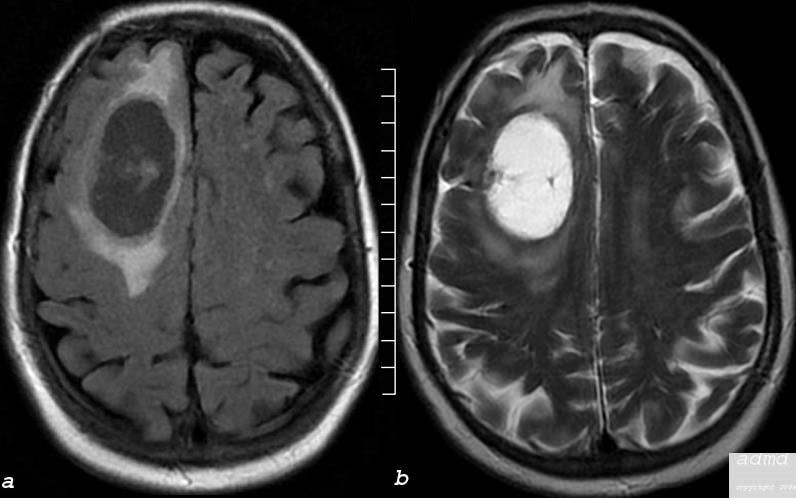
Brain Abscess Caused by Sinusitis |
| The MRI is from a 40 year old female who presents with a headache and has sinusitis which was complicated by a brain abscess.
Image (a) is a T1 weighted axial image taken at the level of the lateral ventricles and shows a mass with an air bubble and a small air fliouid level in the right frontal lobe. Image (b) is a T2 weighted image showing complex fluid in the abscess cavity that is not as intensely bright as the CSF. There is surrounding edema in the brain substance and the black air bubble is again seen. Image c is FLAIR sequence in axial projection that has features similar to th T2 weighted image and image (d) is a coronal FLAIR sequence showing the paracentral location of the abscess. In this image the left maxillary sinus is is totally opacified consistent with the diagnosis of maxillary sinusitis Courtesy Ashley Davidoff MD Copyright 2010 71604.c02 |

|
Cysticercosis |
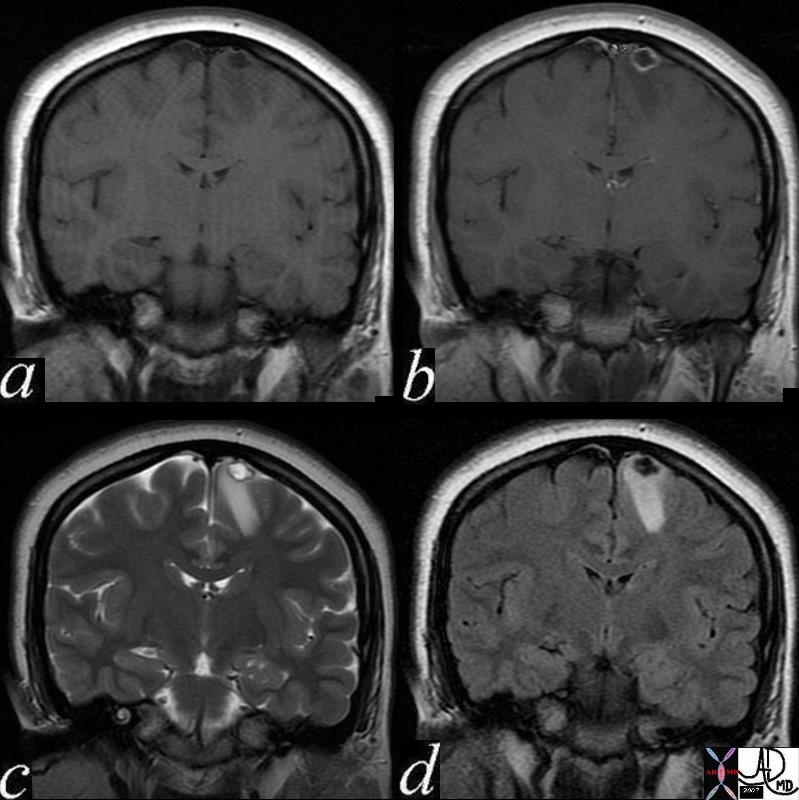
| This 24 year old female presented with seizures
An MRI with gadolinium enhancement suggested a diagnosis of cysticercosis. Image (a) is a pre gadolinium T1 weighted coronal image showing a hypointense focus in the paramedian part of the frontal lobe. Image (b) shows rim enhancement of the lesion. Image (c) is a coronal T2 weighted image that shows a hyperintense centre with a dark rim. A hypointense scolex can be seen as a tiny linear defect within the cavity. Surrounding edema is present in the white matter. Image(d) is a FLAIR coronal sequence and shows a dark matrix and edema in the surrounding white matter. The linear scolex inside the cavity is seen as relatively hyperintense. These finding are consistent with the diagnosis of cysticercosis. Courtesy Davidoff MD Copyright 2010 All rights reserved 71575c02 |
Atrophy

Small Frontal Lobes |
|
The axial CT of the brain of a 50 year old male shows mild bifrontal atrophy as revealed by an increase in the extra-axial space 72736.600 50 year old male brain frontal lobes small frontal lobes atrophy CTscan Courtesy Ashley Davidoff MD |
|
Cystic Metastasis – Squamous Cell Carcinoma |
|
The MRI performed in the axial plane shows a large mass in the right frontal region and the anterior half of the centrum semiovale. Image (a) is an axial image through the vertex of the brain using FLAIR technique showing mostly a cystic type lesion with some internal thick sepatation with surrounding vasogenic edema. Minimal mass effect on the midline is perceived. Image (b) is an axial T2 weighted sequence showing a cystic matrix and surrounding edema The lesion was shown to be a cavitating squamous cell metastasis Courtesy Ashley Davidoff MD Copyright 2010 75408c03 |
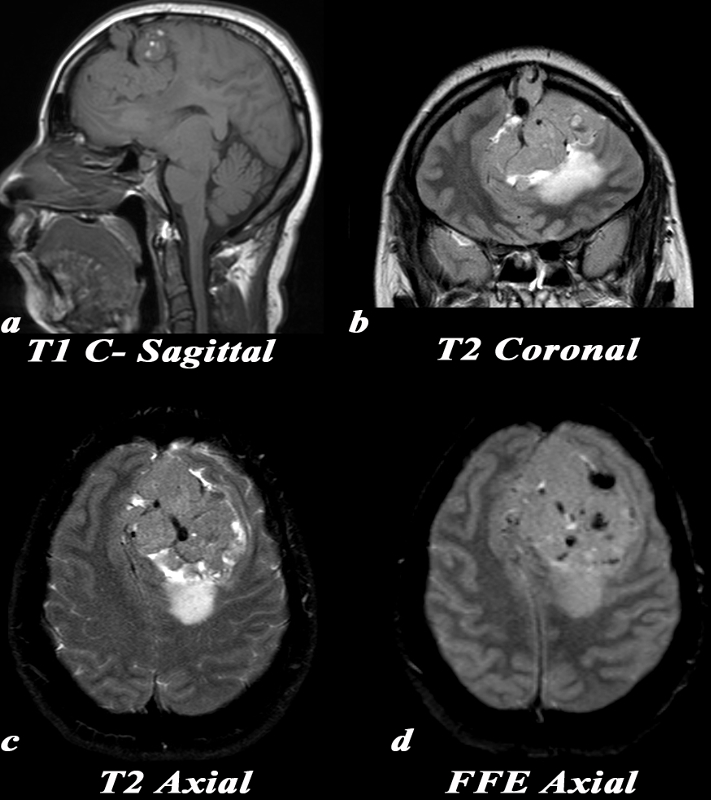
Heangiopericytoma of the Fontal Lobe |
|
This 30 year old pregnant female presented with a constant headache and an MRI was obtained. Note that MR contrast was not given due to her pregnancy. MRI: Because this mass is isointense and large, it can be difficult to distinguish if it arises from within the brain parenchyma (intra-axial), or if it is external to it (extra-axial). Note how the brain tissue is buckled around the mass sagittal T1 (a), and coronal T2 (b), and compressed by it, suggesting that it is extra-axial in location. T1: (a) The mass is predominantly T1 isointense with several areas of high T1 signal which may be related to blood products. A large internal blood vessel is noted. T2 coronal: (b) Notice the aggressive features of this mass which include erosion through the overlying skull and large internal network of blood vessels which are the linear low intensity structures. Increased T2 signal consistent with edema is seen in the underlying parenchyma. The mass itself is isointense to gray matter with central hypointense foci which are consistent with large blood vessels. T2 axial:(c) Mass effect, shift of the midline, internal network of vessels (linear low intensity structures), and T2 bright posterior peritumoral parenchymal edema. FFE: (d) This gradient echo MRI sequence is beneficial for picking up substances which alter the local magnetic field, or paramagnetic substances. These substances cause “blooming” which is a loss of signal, or hypointensity, within and just around them. Note the multiple areas of “blooming” within the mass which can be caused by blood products or calcification. Image Courtesy Elisa Flower MD and Asim Mian MD 97656c.8 |
Leukodystrophy

10 year old with Leukodystrophy |
|
This MRI is from a 10 year old male with known leukodystrophy. The findings on the MRI of the brain (a,b) are characterised by significant changes in the white matter of both frontal lobes. (green arrow), characterised by T2 and FLAIR hyperintensity These findings are consistent with leukodystrophy. Courtesy James Donnelly MD Copyright 2010 All rights reserved 23431c01 |
|
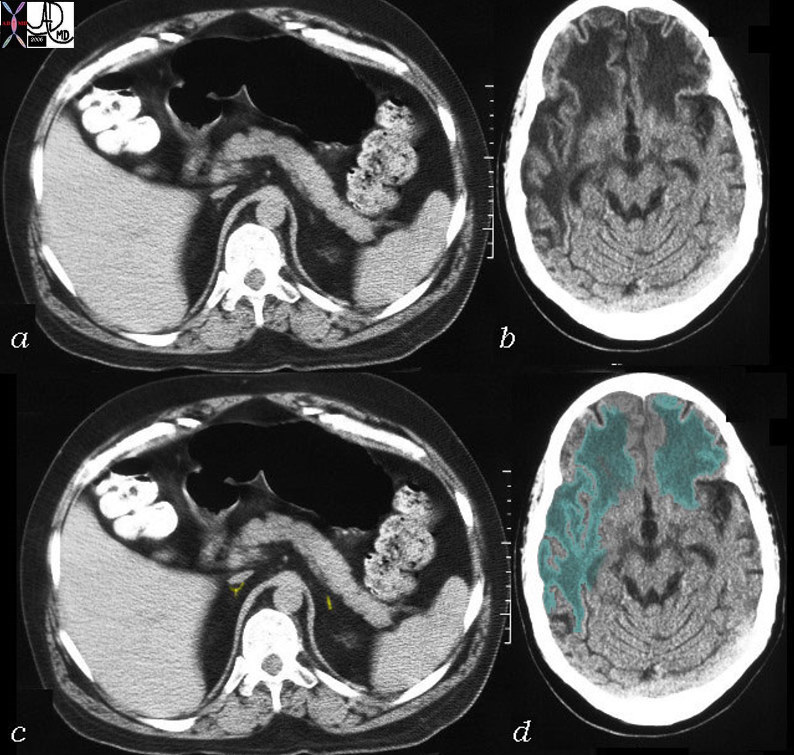
Adrenoleukodystrophy |
|
This CT is from a 26 year old male with known adrenoleukodystrophy. The findings on the CT of the brain (b,d) are characterised by significant changes in the white matter of both frontal lobes right parietal lobe and left parietal lobe to lesser extent. (green overlay) The adrenal glands (a,c) are barely visible but are overlaid in yellow in image (c). These findings are consistent with adrenoleukodystrophy. Courtesy Rebecca Schwartz MD Copyright 2010 All rights reserved 31464c04 |
Middle Frontal Gyrus
The middle frontal gyrus is the second third of the frontal lobe, bound by the superior frontal gyrus and inferior frontal gyrus as well as the precentral sulcus. The middle frontal gyrus Dysfunction is manifested as impairment in working memory as well as general cognitive dysfunction. Diagnosis involves neuroimaging techniques including fMRI. Treatment involves pharmocological attempts at the mitigation of symptoms.
|
Middle Frontal Gyrus |
| 49060 brain abnormal Lateral ventricle putamen caudate nucleus middle frontal gyrus Chronic Infarct Posterior Putamen T2 axial Courtesy Ashley Davidoff MD Uploaded RP |
Inferior Frontal Gyrus
The inferior frontal gyrus is the final third of the frontal lobe, bound by the middle frontal gyrus, inferior frontal sulcus, lateral fissure, and inferior precentral sulcus. Broca’s region of the brain is located within the inferior frontal gyrus. Broca’s region is responsible for speech ability and comprehension. Dysfunction results in aphasia and other speech related difficulties. Diagnosis involves observation of impairment followed by cognitive and neuroimaging tests. Treatment involves speech therapy and routine medical monitoring of the condition.
|
Inferior Frontal Gyrus |
| This axial image of a normal T2 weighted MRI scan shows high intensity CSF anatomy. Courtesy Ashley Davidoff MD 38703c03g code CNS brain CSF normal |
Precentral Gyrus
The precentral gyrus is anterior to the post central gyrus and bordered by the precentral sulcus and lateral fissure. It is the location of the primary motor cortex which is responsible for planning and executing movements. Lesions are the primary source of impairment of the precentral gyrus and cause paralysis of the contralateral side of the body. Neuroimaging is used to determine the origin of the lesion. Treatment includes rehabiliatory therapy.
|
Precentral gyrus |
| 49121 Brain Normal 61 Male Lateral Ventricle Central Sulcus Precentral gyrus Postcentral gyrus T1 Axial Courtesy Ashley Davidoff MD Uploaded RP |